Satellite communication for disaster management
Satellite communication for disaster management
IT-supported management of mass casualty incidents: the e-Triage project
IT-supported management of mass casualty incidents: the e-Triage project
Anton Donner and Javier Mulero Chaves
DLR, Institute of Communications and Navigation, Weßling/Oberpfaffenhofen, Germany
Introduction
The World Health Organization (WHO) gives the following definitions of disasters and emergencies:
“Disasters are events that occur when significant numbers of people are exposed to hazards to which they are vulnerable, with resulting injury and loss of life, often combined with damage to property and livelihoods.”
and
“Emergencies are situations that arise out of disasters, in which the affected community’s ability to cope has been overwhelmed, and where rapid and effective action is required to prevent further loss of life and livelih-ood.” (1)
These definitions imply that emergencies are characterized by limited resources in terms of medical personnel and infrastructure, which underlines the importance of mobilizing regional, supra-regional and/or international help to the affected regions. Effective deployment of this help is crucial but only possible if a common operational picture between authorities, coordination centers, and staff working in the field is rapidly developed.
Upon arrival on site, the first task of a rescue team is to look for injured persons and to assess the situation. For scenarios with many (seriously) injured persons, many countries have foreseen a standard procedure for the initial scouting, known as “triage”. According to it, teams consisting of medical doctors or paramedics classify victims according to different categories (e.g., immediate, delayed, minor, no chance of survival) and attach paper labels to the victims.
Paper-based triage and registration systems are still state-of-the-art, because they are robust and their usage is intuitive. Nevertheless, the main drawback is that information about affected persons remains among the persons themselves, making disaster management considerably more difficult. Data can be duplicated/ aggregated by manually copying triage tags only, which is a laborious and time-consuming process. Moreover, as soon as there is more than one rescue team (organization) involved maintaining different lists, or there is more than one access to the disaster area (which is the typical case for wide-area disaster events with large geographical extension, like earthquakes), registration of injured/affected persons turns out to be a logistic problem since it can only be performed at defined transfer points. Besides, experience has very often shown that injured persons ‘bypass’ the theoretical work flow of the rescue chain (see Figure 1), because passers-by or relatives take them to the nearest hospitals. This effect implies an additional problem, namely a saturation of the geographically nearest hospitals, which very often do not have a communication return channel to coordination centers.
Figure 1: Present work flows and operation control for individual rescue (solid lines and blocks) and MCI (dashed lines and blocks).
Indeed, triage and registration performed at different places by different teams maintaining different lists are indubitably an error-prone approach. It can happen that all later attempts to track the way of single patients, their attendants and transport vehicles are not very successful, although this could be of key interest in scenarios with nuclear, biological or chemical hazards. Last but not least, relatives have a legitimate interest in the whereabouts of their family members.
Communication and dissemination of this information in order to provide coordination centers with an accurate situation overview (i.e. number of victims, injury categories and their location) becomes one of the main challenges to overcome, since the normal medium nowadays for exchanging information are voice-based radio systems.
Key concept
Earlier works have already described concepts for and advantages of IT-supported MCI management, which can be applied not only to operations in the field, but also to emergency rooms of hospitals. A comprehensive overview can be found in (2). Some of these system architectures include wearable sensors with wireless connectivity, e.g. (3), (4); others use radio-frequency identifications (RFIDs) in read/write mode, e.g. (2), (5), which means that data is stored both in the RFID chip and transmitted from a handheld device to a database. The main objective of this article is to describe the e Triage approach (6), which is a research project funded by the German Federal Ministry of Education and Research and which consists of four main elements: autonomous communication infrastructure, electronic data recording, a distributed database system (7), and psychological acceptance research. Outcome of the project will be a demonstrator system for registration of affected persons of an MCI. In more details, the e-Triage system comprises a satellite-based communication system with terrestrial radio cells that can be installed in the field, matching end devices with dedicated application software for the registration of victims, and a distributed, self-synchronizing database system guaranteeing maximal availability without a single point of failure. Main differences to approaches described in literature are:
- Sensors monitoring vital parameters of single patients might be a valuable tool in hospital environments, but for e-Triage the concept decision was to apply a simple classification scheme only.
- Triage tags (registration cards or colored wristbands) are not used as data storage media. Instead, a triage tag is labeled with a unique identifier (ID) in different formats only (RFID, optical matrix code, human readable text). With the ID the patient’s data set can be obtained from the database.
- A distributed database system mapping IDs to persons is a key component of the approach. Not only hardware with optical/RFID scanners can be used to obtain the patient ID, but also notebook or desktop computers may be used for this purpose (with the database software running from external flash drives and the ID typed in with a normal keyboard).
- User terminals are designed primarily for regular rescue services, so that in case of a disaster they are instantly available.
Unique electronic labels remaining attached to victims show advantages for the subsequent rescue chain: due to the contact-free readability it is possible to equip ambulances and doorways of (field) hospitals with scanners which automatically transmit the new location (and/or the geographical position) of the respective person to the control center via various complementary wireless transmission links (see below). Additionally, patients could change their status (e.g., from category II “delayed” to category I “immediate”) and this information is fed into the continuously updated distributed database allowing an operation control to trace how the situation evolves. On site forces can be redeployed and additional forces dispatched on the fields. (Field-) Hospitals can organize their care capacity, call for back-up personnel and send feedback reports to remote coordination centers. Last but not least, information regarding the whereabouts of the victims is easily obtainable and the entire information base is available for a later evaluation since MCIs are always subject to later police investigation.
Data management

Figure 2: Distributed database system (DDBS) concept and synchronization of DDBS instances along the rescue chain.
Albeit the main challenge for the e-Triage system is aggregation of distributed data acquired from many terminals in the field, a fully centralized approach for data storage is not desirable. Rescue operations are temporally and spatially distributed events. Thus, a distributed data management approach has to be applied (see Figure 2). Arriving triage and medical rescue teams have to be able to start working immediately without having to wait for the communication infrastructure to be set up. Furthermore, all the collected data needs to be forwarded to local and remote decision makers automatically. As an integral part of this architecture, network outages or node failures have to be anticipated. Thus, the underlying storage technology will be a distributed database system (DDBS), which has to cope with a variety of different communication technologies, including terrestrial wireless and satellite links with different bandwidths. A basic assumption for the design is that, on the one hand, the network topology might change at any time. On the other hand, all involved communication links are not reliable so that intermittent network outages might occur (e.g., end devices leaving the coverage area of the locally installed radio cells). Nodes of this DDBS are installed in all mobile user terminals (tablet-PCs), at communication nodes (OSECEs), and in the remote area. The DDBS discovers joining and leaving nodes, and (re-)joining nodes have to be synchronized with the core DDBS. This design supports even scenarios with no network connectivity at all: it is possible to synchronize database nodes by exchanging flash memory cards.
Communication

Figure 3: e-Triage communication suitcase (on-site emergency communications equipment, OSECE) consisting of an Inmarsat BGAN satellite terminal, a GSM pico cell, and a WLAN router (9).
An electronic registration system for MCIs requires wireless communication services, and since local infrastructures may not exist at all or can be destroyed, it is of paramount importance that at least a temporary communication system is set up. Even if functioning networks exist, it is most likely already saturated by the affected persons using their mobile phones. For rescue missions in less densely populated or less developed or seriously destroyed countries satellite phones (e.g., Globalstar or Iridium) are commonly used during the first hours/days. The idea of backhauling terrestrial cellular networks via a long-haul satellite link is not new and commercial products already exist. An example is Emergesat by Thales Alenia Space which has been designed to fit into a container for air freight. Disadvantage of this solution is that it is rather bulky and transport into an affected area can be rather challenging. The development of a more flexible and faster deployable solution has been initiated in the WISECOM project (8) and is currently continued within e-Triage. The basic design goal is that the complete on-site emergency communications equipment (OSECE) fits into a hand-luggage size suitcase. The chosen satellite technology is Inmarsat BGAN, which is globally available but offers limited bandwidth only, and the resulting suitcase prototype is 56cm x 35cm x 23cm, including a battery pack for a few hours runtime (9). The BGAN terminal itself needs only to be taken out of the suitcase, and the antenna can be easily pointed to the satellite within a few minutes.
A second more powerful OSECE system is currently under development for use in mobile coordination centers, which is based on a commercial Very Small Aperture Terminal (VSAT) satellite system and which offers more capacity and wider terrestrial coverage. Manual alignment of the antenna reflector (diameter ca. 1 m) is not an option for this application, so the decision was to use a self-aligning antenna unit which can be mounted on a suitable vehicle.
The quasi-stationary OSECE nodes include several base-stations for different wireless technologies:
- WLAN: Data communication as well as Voice over IP (VoIP) calls can be provided by WLAN access points. For the registration of affected persons WLAN is the preferred medium since it offers sufficient bandwidth for many terminals in parallel.
- GSM/GPRS: These well-known standards allow voice and data communication. GSM cell phones are inexpensive and available all over the world, which in turn means that in most cases the access to the temporary GSM service has to be restricted to avoid network congestion. Then again, a GSM base-station can be configured so that unknown phones are booked into the network in a listen-mode only, which is an excellent possibility to distribute information or warning messages among the population in the area. A major disadvantage of GSM is the missing group call functionality. General packet radio service (GPRS) is the secondary medium for data exchange in the e-Triage concept.
- DECT: Digital Enhanced Cordless Telecommunications (DECT) is suitable for voice communication in vicinity of the local coordination center.
- TETRA: The PMR standard TETRA will not be part of the final demonstrator system, but is currently under study within the project.
The different terrestrial wireless technologies supported by an OSECE are depicted in Figure 4. Note that two or more OSECEs connected via WLAN in bridged mode can be deployed in the field with only one having backhaul connectivity.
Figure 4: Fully deployed e-Triage communication infrastructure.
Conclusion
This paper has given a brief description of the architecture of the e-Triage system and the challenge to manage data in MCIs. Although earlier and other current works have studied single components of electronic MCI management, a unique feature of e-Triage is that for the first time a coherent overall concept consisting of mobile devices, communication infrastructure, and data management is under development. Another unique feature is that all developments, ranging from hardware selection to graphical user interface implementation, are accompanied by a team of psychologists, ensuring that all components are self-explanatory and can be used intuitively without causing additional stress. At the time of writing this article the system is under implementation and a series of real-live trials will start from January 2011.
Public safety communication means in most cases voice communication (group calls) using dedicated PMR networks, which are designed for closed user groups with partly specific confidentiality requirements. Introducing data communication to public safety requires appropriate preparation, which means that one may not rely on the availability of public (commercial) terrestrial networks only. With our satellite-based communication facilities flexible data services can be provided plus the possibility to quickly establish point-to-point telephone services in case of extreme disasters. It is important to remark that even without a backhaul link all the services provided in the disaster area are available, so that the rescue operation will not be affected
References
- B. Wisner and J. Adams, Eds., Environmental health in emergencies and disasters: a practical guide. World Health Organisation (WHO), Jul. 2003. [Online]. Available: http://www.who.int/water_sanitation_health/hygiene/emergencies/emergencies2002/en/
- S. Nestler, M. Huber, and G. Klinker, “Hybrid approach for management of patient-related information in mass casualty incidents,” Technische Universität München, Technical Report, Oct. 2009, TUMI0926. [Online]. Available: http://ar.in.tum.de/Chair/PublicationDetail?pub=nestler2009hybrid
- T. Massey, T. Gao, M. Welsh, J. H. Sharp, and M. Sarrafzadeh, “The design of a decentralized electronic triage system,” in American Medical Informatics Association (AMIA) Annual Symposium Proceedings, 2006, pp. 544–548, PMCID: PMC1839501. [Online]. Available: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1839472/pdf/AMIA2006_0429.pdf
- T. Gao and D. White, “A next generation electronic triage to aid mass casualty emergency medical response,” in Proceedings 28th Annual International Conference IEEE Engineering in Medicine and Biology Society (EBMS), New York City, USA, Aug./Sep. 2006.
- S. Inoue, A. Sonoda, and H. Yasuura, “Triage with RFID tags for massive in-cidents,” in RFID Handbook: Applications, Technology, Security, and Privacy, S. A. Ahson and M. Ilyas, Eds. CRC Press, Mar. 2008, ch. 27, pp. 329–349.
- A. Donner, C. Adler, M. Ben-Amar, and M. Werner, “IT-supported manage-ment of mass casualty incidents: The e-Triage project,” in Proceedings 5th Future Security Research Conference, Berlin, Germany, Sep. 2010.
- C. Tang, A. Donner, J. M. Chaves, and M. Muhammad, “Performance of database synchronization via satellite,” in Proceedings 5th Advanced Satellite Multimedia Systems (ASMS) Conference and 11th Signal Processing for Space Communications (SPSC) Workshop, Cagliari, Sardinia, Italy, Sep. 2010, pp. 455–461.
- E. H. Fazli, M. Werner, N. Courville, M. Berioli, and V. Boussemart, “Integrated GSM/WiFi backhauling over satellite: Flexible solution for emergency communications,” in Proceedings 67th Vehicular Technology Conference (VTC2008-Spring). Singapore: IEEE, May 2008, pp. 2962–2966.
- À. V. Estrem and M. Werner, “Portable satellite backhauling solution for emergency communications,” in Proceedings 5th Advanced Satellite Multimedia Systems (ASMS) Conference and 11th Signal Processing for Space Communications (SPSC) Workshop, Cagliari, Sardinia, Italy, Sep. 2010, pp. 262–269.
Emergency.lu Solution
Emergency.lu Solution
Marianne Donven, Luxembourg Ministry of Foreign Affairs
Benjamin Hourte, HITEC Luxembourg S.A.
Alan Kuresevic, SES Astra TechCom
Sven Mertes, Luxembourg Air Rescue
Context and motivation
January 12, 2010: Haïti has just been hit by an earthquake of historic magnitude. Hours later President René Préval is walking through the debris of the devastated capital Port-au-Prince: “My palace collapsed… I have no connectivity for my cell phone to even call somebody for help…”.
January 14, 2010: Urban Search and Rescue (USAR) teams from Luxembourg arrive in Port-au-Prince, together with humanitarian workers from France and Belgium.
January 15, 2010 (in the morning): USAR teams, with their dogs, are still not able to leave the airport and likewise hindered to start their mission. Lacking telecommunications, among other requirements, are identified as a cause of poor coordination.
After a natural disaster of such proportion the first 72 hours are crucial to save lives. This is all the more true in an urban context. Not to blame anybody, but precious time was lost in Haïti because the necessary tools for quick and reliable communication were not in place in order to coordinate and deploy USAR teams as they arrived.
Upon the return of the USAR teams to Luxembourg, a debriefing session with all participants in the Ministry of Foreign Affairs allowed to sketch out a first rough draft of what is presented here as emergency.lu. This initiative is intended to bring added humanitarian value through faster and more reliable telecommunication services in the first few hours following a natural disaster, a segment of emergency relief still insufficiently covered today. In order to provide such a solution, emergency.lu bundles the already available equipment and services from three different providers:
- Luxembourg Air Rescue’s (LAR) air transport capacity to reach any destination worldwide within less than 24 hours,
- HITEC Luxembourg’s portable Nomadic Satellite Communications (NoSaCo®) system providing end user services for voice, data and video transmission via the internet (for on-site coordination between intervention sites and global transmission, respectively),
- Société européenne des satellites’s (SES) global satellite capacities for satellite based broadband internet connectivity.
Under the coordination of the Luxembourg Ministry of Foreign Affairs (Directorate for Development Cooperation and Humanitarian Action ), Emergency.lu has been established as a public private partnership with the objective to satisfy the telecommunication needs of the international humanitarian community in the immediate aftermath of a natural disaster.
Emergency.lu approach
The Emergency.lu approach has been defined to propose a set of services that can be used without delay by experts and rescuers arriving on site. The lack of coordination during the first hours after a crisis is a real difficulty to get the relevant information to prepare and coordinate the help. The existing European (ECHO) and International (OCHA) structures, both defined to organise coordination, are already proposing the appropriate mechanisms to request and organise help. The need of status information from the crisis site is mandatory to prepare the relevant activities.
Communication is very important in this first step. The experts going on the site are not telecommunication engineers but experts in needs assessment and medical care. They should have access to efficient tools for conducting situational analysis. Here Emergency.lu is providing an approach creating broadband communication and additionally offering a set of services that can be directly used by the experts. The existing TAST and AHP modules proposed by the UN and ECHO can use Emergency.lu. The service approach also includes the end-devices that can be directly and intuitively used by these experts. The equipment deployed on site, NoSaCo (Nomadic Satellite Communication), is creating a Service Point of Presence (SPoP, Figure 1). It is composed by:
- a satellite communication module, easy to point even by non telecommunication experts thanks to a sound and visual pointing system,
- video cameras to provide picture and video streams,
- sensors to capture and transfer environmental information,
- voice over IP phones to communicate locally, with the operation centre or with the other deployed SPoP,
- ruggedized computers to manage the information and draw maps or needs assessments.
The Haiti crisis has drastically shown also that for such a large crisis the deployment of a central communication point is not enough as the help will be spread along all the theatre of operations. The creation of several SPoP can help to distribute also the coordination and the collection of status information. A permanent assessment of the rescue and humanitarian activities can thus be realised, receiving constant information from different locations of the crisis site.
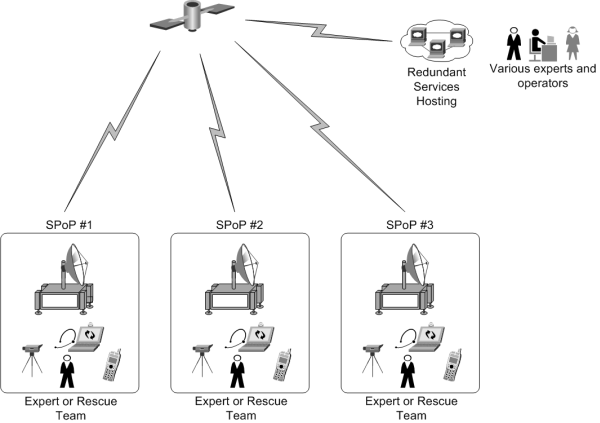
Figure 1: SPoP deployment
Receiving ample information can be a real add-on also for the analysis of the situation. Indeed, the collection of pictures, sensor information or video clips from the crisis site allows different experts, specialised in different areas, to make their proper analysis. For example, water quality specialists can receive in their laboratory the water analysis gained on site through sensors.
To efficiently collect this wealth of information, the NoSaCo terminals are also equipped with software for collecting information from the end-devices (cameras, sensors or computers), and storing and sharing it with the other SPoP or with the Service Hosting. This distributed architecture allows an advanced management of the resilience, security and quality of service, ensuring that the local collection and access to information is still possible even when no communication to the Service Hosting is possible. Once the communication is restored, synchronisation processes are sharing automatically the information with other SPoP and in the Service Hosting. The onsite experts or the operators do not have to take care of the technical elements and can focus on their primary mission.
Technical architecture and technologies
The technical architecture behind the Emergency.lu platform relies on three separate layers (Figure 2).
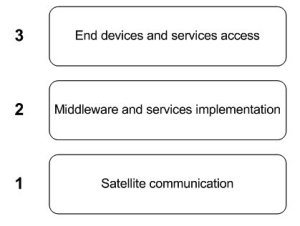
Figure 2: Architecture layers
Similar to the OSI layers, these layers provide different levels of abstraction, from the satellite telecommunication to the final delivery of a service to experts and other users.
Layer 1: Satellite communication
The overall telecommunication concept relies on the creation of three geographically distributed hubs. With the similarity to the OSI Layer representation, the Satellite communication layer can be compared with the physical layer. The hubs will maximize service availability and resource usage efficiency by implementing advanced techniques such as DVB-S2 / ACM and LDPC FEC coding on outbound, MF-TDMA and 2D 16-State coding on inbound. In addition, QoS management and TCP optimization will guarantee a good service experience to the end user.
From a satellite connectivity perspective, the teleports hosting the hubs are selected to enable up-linking to a designated subset of SES satellites that will provide a true global coverage. As presented in Figure 3, three hubs geographically distributed over the world give access to enough satellite beams from SES fleet in order to provide both C and Ku band global coverage.
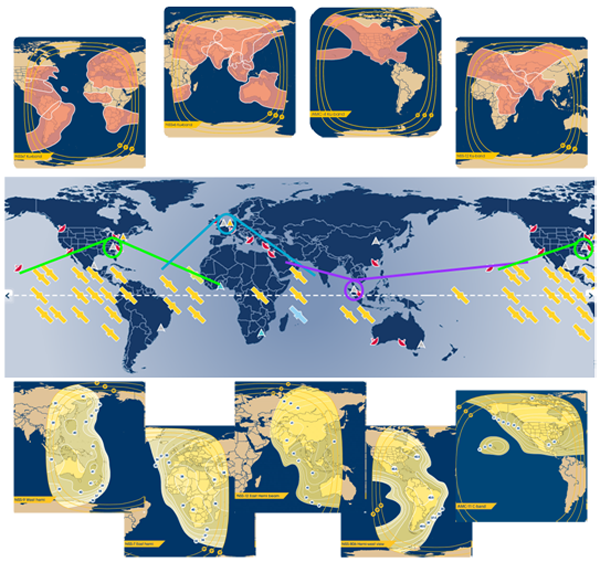
Figure 3: True global coverage (C band below – Ku band above)
This additional flexibility on the frequency side will allow tailored solutions from a link budget point of view. Furthermore, relying on a single satellite operator also brings economy of scale and allows for easy management of a global satellite service through a single interface.
From and between the teleports, IP connectivity will be ensured to the Service Hosting and the global Internet. Furthermore, the Internet connectivity allows the establishment of VPN (Virtual Private Network) connections and dedicated QoS (Quality of Service) for remote crisis centers, NGO headquarters or any other management entities. Security and privacy can be provided through encryption of the traffic. Additional security can be considered at application level.
On the crisis site, NoSaCo terminals are deployed on site to create an IP connection with the relevant hub. This connection will be used to create and deploy the service. The technologies implemented in the NoSaCo terminals are obviously highly tainted by the technologies implemented in the hubs. The main concept of these terminals is to integrate the modem into a compact, light weight and easy to deploy module. The compactness of the terminal will allow its transportation in small planes not requiring a long preparation time (Figure 4).

Figure 4: NoSaCo terminal
Layer 2: Middleware and services implementation
From a service layer point of view, the two hosting platforms are implemented in Emergency.lu to deliver the service to the users. The service implementation is however not only relying on the central hosting but on distributed service implementations (Figure 5). Each NoSaCo terminal is integrating a small part of the service allowing a local relay of the service. The direct advantage of this distribution is the possibility for the service to work whenever the satellite connectivity is present or not. A kind of off-line mode is created as a result.
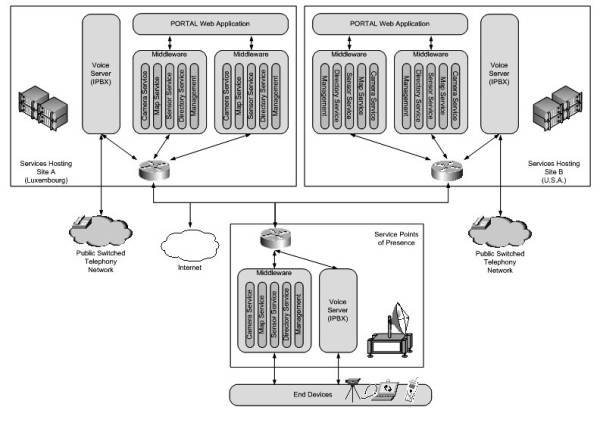
Figure 5: Service Architecture
The services supported and provided are basically:
- Voice communication using SIP based Voice over IP communication: Each Service Hosting is implementing an IPBX with dedicated connection to PSTN and offering a link to small IPBX implemented into the NoSaCo terminals.
- Camera Service: Collection and sharing of imagery and video streams provided by the included cameras or via manual upload.
- Map Service: Repository of tactical maps that can be accessed and drawn by different frontend applications.
- Sensor Service: Collecting, analysing (based on thresholds), storing, and sharing sensor data. Typical sensor information can be gas and pollution concentration, humidity or temperature. This service is also managing the dynamic localisation of entities provided currently by GPS.
- The Directory Service is managing the contact information that is used for voice communication as well as an inventory of devices or components and their logical organisation.
- The Management Service is finally the back end component that is taking care of tracking the other middleware nodes, the auto-configuration and the security of the information.
To ensure a convenient user experience, all services are using a self-discovery concept via IP multicast mechanisms and are directly managing their communication and synchronisation without any intervention from the users.
Layer 3: End devices and services access
To provide an intuitive access to the services, the NoSaCo terminals include a set of equipment that is used to collect information (Video cameras, sensors) or to directly interact with the services (Voice over IP phones, ruggedized computers). These end-devices are pre-configured to work with the NoSaCo terminal and, as a result, ready to operate in any place.
As stated before, the terminal has been implemented in order to facilitate its transportation and make its installation as simple as possible to anyone with a minimum amount of technical knowledge and skills. The use of the service is made as convenient as this, using intuitive, specifically designed applications.
For the usage on the crisis site, the ruggedized computers are equipped with a tactical application that is offering an access to the different services via a touch screen interface (Figure 6). This interface is using the gesture recognition, now popular in the mobile areas and specifically interesting for ergonomics. Touch screen interfaces are facilitating the handling of the applications as no pointing devices like mouse or trackball are required.

Figure 6: Tactical client Interface
On the other hand, in the crisis center or headquarters, a web portal can be used as user interface (Figure 7). The portal provides access to the same services (Voice, Video, Sensor, Maps and Directory). Relying on Web 2.0 technologies, it can be accessed from different places in the world like in laboratories or crisis rooms in different capitals.
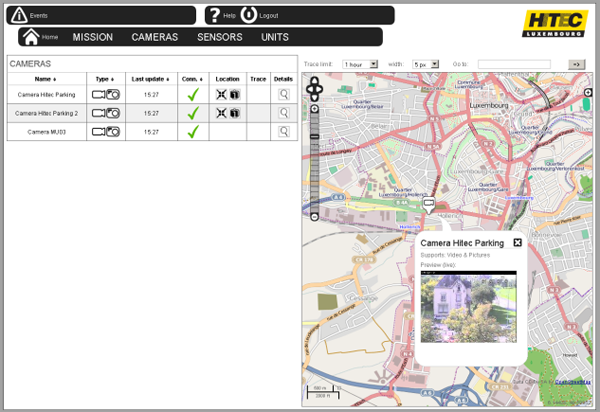
Figure 7: Portal Screenshot
Deployment scenarios and conclusion
As mentioned before, the Emergency.lu approach has been designed with the intention to improve the situation on two main levels: First, reduce the duration of transport of the very first teams to any major crisis scene and second, provide adequate communication means right from the beginning.
To meet these objectives, the consortium has decided to include air transportation in the solution. Through a fleet of LearJet’s, ready to leave Luxembourg within the hour, and with operational and medical staff on a 24 hours a day duty schedule on the airport, Luxembourg Air Ambulance (LAA) can ensure the required reactivity.
Although LAA has over 20 years experience in supporting disaster relief and humanitarian missions with fixed wing and rotor wing aircrafts as well as medical teams, this more global approach requires an impeccable planning involving all the partners. At the airport, a controlled storage is kept constituted by NoSaCo units, food and beverage to guarantee autonomy of the team for 15 days, basic medical supplies for the team and required logistic equipment (i.e. tents, generator).
Frequent trainings, exercises and pre-emptive maintenance are organised to maintain the Emergency.lu platform on a ready to operate status.
Besides the technical readiness, the qualification of personnel involved in these rescue missions is crucial. Procedures have been designed to optimize the collaboration between the different actors, and training is recurrently organised. For an optimal effectiveness of the team, the pilots have been trained to install and operate the NoSaCo installation on site. They are able to give instructions to the local teams and function as on-site support. All team members have received in depth crisis management education and have experience in disaster relief missions.
The emergency.lu intervention team is completed by one or more medical staff , with the primary objective to ensure the medical support for the crew and to support the medical assessment of the situation.
Finally, in best case, the unit is completed with one or more experts for needs assessment assigned by international organisations, i.e. UN (OCHA) or EU (ECHO/MIC). Through the network of partner operators in Europe, LAA can rapidly transport these experts from within Europe not to delay the departure of the mission.
It is very important to point out that the Emergency.lu solution is not intending to replace any existing mechanism or intervention teams, but that it should be seen as a valuable and helpful support. This service is planned to be offered to all international and national organisations. It has to be clearly stated that the solution will work hand in hand with known UN forces.
Once the system is deployed, it can be decided either to dissolve the unit and return to Luxembourg with the equipments, or one can consider building a more permanent communication infrastructure, potentially through an increased amount of NoSaCo units. This last option considers that the effort to support the on-site population in the first hours can also be maintained to assist in the reconstruction of local infrastructures.
PLATON - Trusted Unified Communication & Collaboration (UCC) in health or disaster projects
PLATON - Trusted Unified Communication & Collaboration (UCC) in health or disaster projects
Ingo Liedtke, T-Systems International GmbH, PDC Engineering, Germany
Introduction
Flooding in Benin, Earthquake in Haiti, Cyclone Mick swept over Fiji's main island: humanitarian aid and emergency relief teams are more and more in need of a structured, secure information flow through all phases of the disaster management cycle. Additionally, there has to be a solution to deliver limited specialist resources with a virtual worldwide support. T-Systems PLATON services have a suitable answer.
Disaster management in the future – 5C “Collaboration”
As the latest history has already shown: Disasters are increasing. Due to that more and more qualified specialist resources are required on site as well as in project coordination. In many health and disaster projects uncoordinated processes are posing severe problems. Collaboration across different international institutions and local teams does not work well. The activities are very often lacking in transparency, resulting in decreased efficiency of international team work. That means an unnecessary increase in the need for resources and thus higher costs per saved life . Or, even worse, more time to the real rescue is elapsing.
PLATON Services offer support with a virtual specialist resource. This means that the information flow is structured, transparent and traceable if needed to all participants anytime and anywhere. The virtual “Task Force Disaster“ team can effectively support the local team via video, voice, chat and data.
As the Greek philosopher Platon has astutely observed, “the beginning is the most important part of the work”.
The PLATON system
With PLATON (PLATform for Orchestrated Networks), T-Systems offers an Internet-based platform for collaboration cloud services, including all desired functionalities at the highest security level for worldwide teamwork in real-time. Experts can discuss and work together on e.g. an urgent project issue or even on sensitive patient data from the health care field. Participants collaborate in a closed circle absolutely untroubled in virtually tap-proof project rooms installed separately for every single project through secure interfaces where intellectual property and data integrity are protected by precisely defined access rights.
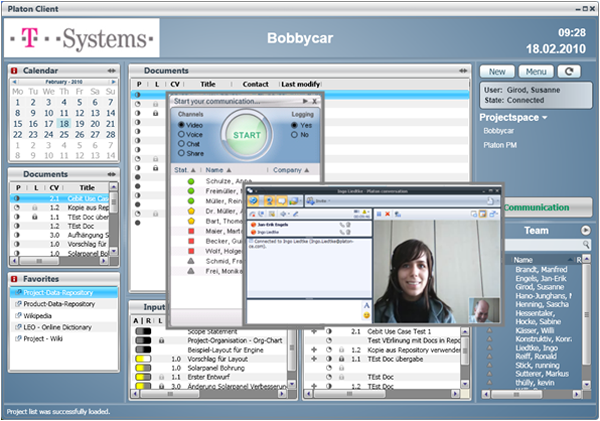
Figure 1: PLATON „virtual“ project room
The advantage of the self-sustaining and secure platform is that the participants in across-company project teams do not have to open their IT systems to each other. Client software with 2-factor authentication on a USB stick with a smart card and a PIN assures secure access of the team members from any place in the world that can be connected to the Internet. All documents, project plans etc. are up to date and seamlessly documented at all times and available for across-continent and across-company project work.
Due to integrated function of Unified Communication and Collaboration (UCC), PLATON users can access all means of communication via their PLATON desktop client, i.e.
- E-mail,
- presence-information,
- data-sharing,
- phone,
- video etc.
to ensure efficient coordination and focused team work.
PLATON automatically updates participants on the current work situation. Ideas, plans and changes can be presented, discussed, modified or discarded without any delay.
Manufacturers and suppliers can communicate necessary product changes instantly, thus speeding up implementation. The virtual meeting room unites team members from different companies and locations in a short time of about 48 h to create real value added networks.
PLATON protects intellectual property and ensures efficient collaboration. PLATON project teams can grow dynamically and change on demand to best suit real-time requirements. This means reduced expenditure of time and resources. The easier it is to quickly integrate different specialists to deal with new project developments, the better the final result. Fewer mistakes mean fewer corrections, less waste, less production downtime and fewer product recalls. T-Systems is prepared to modify the PLATON meeting room to suit individual needs and expert coaches are available upon request.
PLATON – Online surgery for health care and disaster relief
PLATON brings the physician specialist competence to the patient and not vice versa.
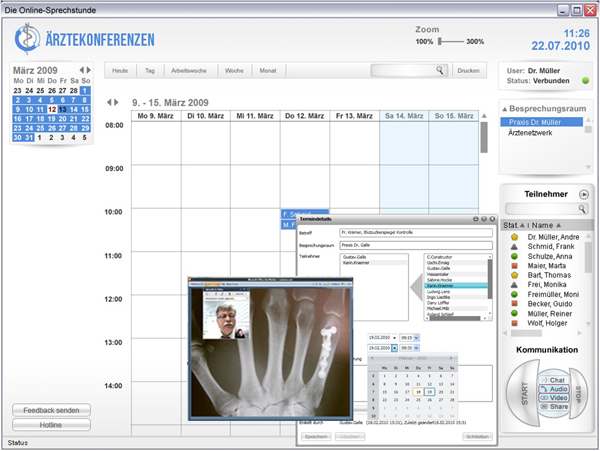
Figure 2: PLATON Health Client “physicians conference - online surgery”
As an example the physician and the patient “meet” each other in a secured, virtual surgery for a video conference. The phyisician takes his data and application and can online discuss the laboratory values, therapy plan modification or X-ray photograph with the patient. The “online-surgery” can be opened for another medical specialist, if a second opinion is needed. They can discuss without media discontinuity and the data does not leave the physician’s PC. The specialist only sees the display of the data. The physicians’ and specialists’ competences can be virtualized and provided in any location, thus easing the communication and saving time and money. Of course the online surgery cannot replace the real surgery, but is in many cases faster and more efficient as usual low-up appointment for a discussion about e.g. laboratory data.
In particular this applies to local disaster situations where specialists are not available on site. With the PLATON services T-Systems can supply a virtual competence center anywhere, anytime, as soon as the internet connection is available on the ground.
PLATON – A new collaborative working model
In a disaster situation the human resources are very likely to be limited and helpful information has to be up-to-date at any location. The PLATON working model supplies the information flow with its structure. Larger data will be sent by an asynchronous process, but is tracked and version-controlled by PLATON. If rapid information is needed, the project members will discuss it via chat in the secure project room with the team members.
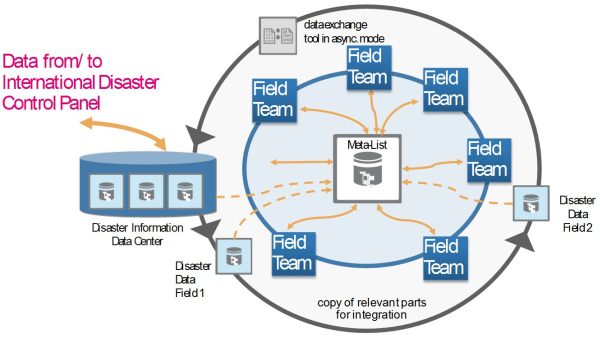
Figure 3: New Collaborative working model - all information flows are encrypted
If certified or uncertified information from the source “crowd” has to be integrated, PLATON can react in a flexible way. As an idea the crowd information will be integrated and structured for example by a data coordinator. This will enhance the quality of information and so the quality of help.
Contact
Ingo Liedtke
T-Systems International GmbH
Systems Integration
Project Delivery Center Engineering
Senior Sales Consultant trusted UCC/PLM
+49 711 972 - 43686 (Tel.)
+49 18053344918366 (eFAX)
+49 160 820 97 43 (Mobil)
E-Mail: ingo.liedtke [at] t-systems.com
Internet: http://www.t-systems.com
https://servicenet.t-systems.de/plm
https://servicenet.t-systems.de/platon